In Slovenia, colon and rectal cancer (colorectal cancer) accounts for around 6 percent of all newly diagnosed cancer cases. Its frequency begins to increase at the age of 40 and is highest after the age of 60.
COLON CANCER: General | Symptoms and Diagnosis | Treatment and Prognosis | Questions and Answers | Sources/references
About 5 percent of people with colon or rectal cancer have more than one colorectal cancer at the same time. People with a family history of colon cancer have a higher risk of developing cancer. The presence of familial polyposis or a similar disease in the family also increases the risk of developing colon cancer. People with ulcerative colitis or Crohn's disease have a higher risk of developing cancer. The risk is related to the patient's age at the onset of the disease and its duration.
Nutrition also plays a vital role in the risk of colon cancer, but the exact data on this is not known. People at higher risk live in bigger cities and eat foods typical of Western countries. Such a diet contains little fiber, animal protein, fat, and processed carbohydrates, e.g., sugar.
Image: appearance of colorectal cancer with a colonoscopy examination

The risk is probably reduced by foods rich in calcium, vitamin D, and vegetables, such as Brussels sprouts, cabbage, and broccoli. Taking acetylsalicylic acid every other day probably also reduces the risk of colon cancer, but this is not recommended because there is not enough data available.
Video content: how does colon cancer develop?

Colon cancer usually begins as a button-like growth on the surface of the intestinal lining or a polyp. As the cancer grows, this change begins to invade the intestinal wall. It can also invade neighboring lymph nodes. Because blood drains from the intestinal wall to the liver, colon cancer tends to spread (metastasize) to the liver shortly after invading neighboring lymph nodes.
Symptoms and diagnosis
Colorectal cancer grows slowly, and only after a long time does the tumor become large enough to cause symptoms. Symptoms depend on the type, location, and spread of the cancer. The upper (right) column has a large diameter and a thin wall. Because its contents are liquid, the blockage occurs only late in cancer development. A tumor in the ascending colon can grow so large that the doctor feels it through the abdominal wall. However, the patient's only symptoms may be fatigue and weakness due to anemia.
The downward (left) colon has a smaller diameter and a thicker wall, and the mud is semi-liquid. Cancer typically surrounds this area of the colon like a ring, causing alternating heartburn and frequent bowel movements. Because the lower colon is narrower and has a thicker wall, cancer is more likely to cause obstruction earlier. A person seeks medical attention for abdominal cramps or severe abdominal pain and constipation. There may be signs of blood in the stool or mixed with blood, but often, no blood can be seen; laboratory tests are required to prove blood in the stool.
Video content: 6 typical symptoms of colon cancer
Cancer mostly bleeds, usually slowly. In rectal cancer, the first symptom is often bleeding during bowel movements. A doctor thinks of cancer whenever a patient bleeds from the rectum, even if they have hemorrhoids or diverticular disease. With rectal cancer, the patient may experience painful defecation and the feeling that the rectum does not empty during defecation. Sometimes, even sitting is painful. Often, however, the patient does not feel any pain until the cancer has spread to tissues outside the rectum.
As with other types of cancer, regular screening tests contribute to its early detection. Even small amounts of blood can be detected in the stool with simple and inexpensive tests. For the results to be accurate, the patient eats food with a lot of fiber and no red meat for three days before the examination. If this screening test detects the possibility of cancer, further investigations are required.
Image: Colonoscopy, a procedure for examining the colon and rectum.
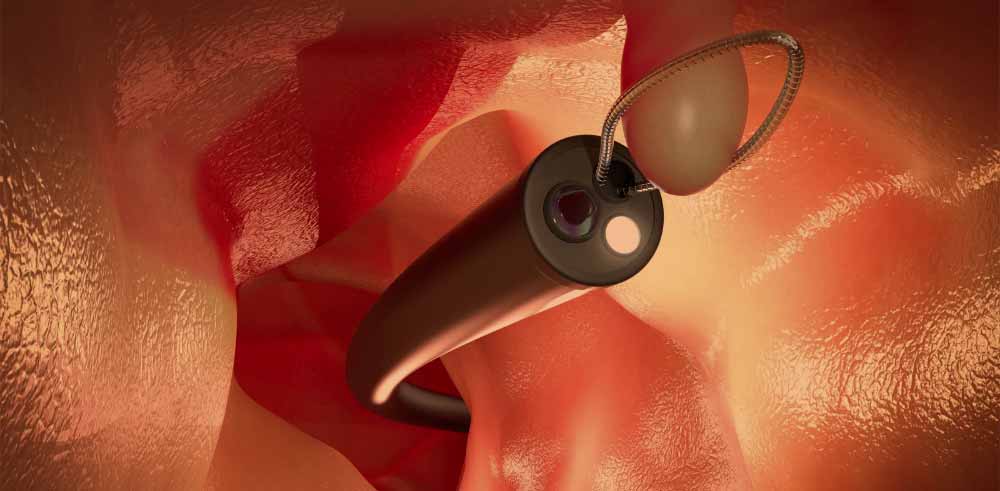
Before the endoscopy, the intestine is emptied, often with solid laxatives and numerous enemas. About 65 percent of colorectal cancers can be seen with a flexible viewing tube, the sigmoidoscope. If they see a polyp that could be cancerous, the entire colon is examined with a colonoscope that reaches further. Some growths that look cancerous are removed with surgical instruments inserted through the colonoscope; others must be removed by ordinary surgery.
Blood tests can help make a diagnosis. In 70 percent of people with colorectal cancer, a high level of carcinoembryonic antigen is found in their blood. If the level of carcinoembryonic antigen is high before the surgical removal of the cancer, it may be low after the operation. In this case, the antigen level can be monitored during the patient's follow-up examinations. A rise in the level again indicates a recurrence of the cancer. Carcinoembryonic antigens are similar to other antigens, CA 19-9 and CA 125, which can also be measured.
Treatment and prognosis
The primary method of treatment for colorectal cancer is the surgical removal of a large area of the affected intestine and adjacent lymph nodes. About 70 percent of people with colorectal cancer are suitable for surgery. In 30 percent of people who cannot undergo surgery due to poor health, some tumors can be removed by electrocoagulation. The procedure otherwise relieves symptoms and prolongs life, but recovery is unlikely.
Video content: the best ways to treat colorectal cancer
In most cases of colon cancer, the cancerous intestine is surgically removed in 1 second and free! Join the ends. For rectal cancer, the type of surgery depends on how far the cancer is from the buttock and how deep it has invaded the rectal wall. After the complete removal of the buttocks and rectum, the patient will have a permanent colostomy (a surgically created opening between the colon and the abdominal wall). In a colostomy, the contents of the large intestine are emptied through the abdominal wall into a colostomy bag. Only part of the rectum is removed when possible, leaving the rectal protuberance and buttock intact. The rectal protrusion is then sutured to the rest of the colon. Radiation therapy after surgical removal of visible rectal cancer can help control the growth of any remaining tumor, delay
|
Cancer spread and survival |
|
|
The spread of cancer |
Five-yearly survival |
|
Cancer only in the intestinal lining |
90% |
|
Cancer that invades the muscle layer of the intestine |
80% |
|
Cancer that has spread to the lymph nodes |
30% |
Disease recurrence and improve the chance of survival. For people with rectal cancer and one to four cancerous lymph nodes, the most successful treatment is a combination of radiation and chemotherapy. In people who have more than four cancerous lymph nodes, this treatment is less effective.
For colorectal cancer that has spread and cannot be cured by surgery alone, postoperative chemotherapy with fluorouracil and levamisole can prolong the patient's life, but the cure is still rare. When colorectal cancer has spread so far that it can't be removed entirely, surgery to relieve the bowel obstruction can ease symptoms. Such patients usually survive for only about seven months. When the cancer has spread only to the liver, chemotherapy drugs can be injected directly into the artery that supplies the liver.
Video content: showing the rates of colorectal cancer.
By surgically inserting a small pump under the skin's surface or with an external pump worn on the waist, the patient can move during the treatment. Although this treatment is expensive, it can be more effective than regular chemotherapy; however, additional research is needed. When the cancer has spread outside the liver, this approach has no advantage.
After the complete removal of colorectal cancer, most experts recommend two to five examinations of the rest of the intestine with a colonoscopy every year. If no signs of cancer are detected during these examinations, the patient is further examined every two to three years.
Questions and answers
What are the first signs of colon cancer?
- change in bowel function and bowel habits,
- blood in the stool or on it during defecation,
- Diarrhea, constipation, or a feeling that the bowel does not empty,
- abdominal pain and pain or cramping that won't go away
- weight loss, but it is impossible to determine why[1].
Is colon cancer curable?
Colon cancer is a very curable or often completely curable disease if it is localized only in the intestines. Surgery is the primary form of treatment, resulting in a cure in approximately 50% of patients. However, the recurrence of colorectal cancer after surgery is a significant problem and is often the ultimate cause of death[2].
How does colon cancer usually start?
Most colon and rectal cancers begin as growths on the inner lining of the colon or rectum, called polyps. Polyps are quite common, especially as people age, and most are benign or non-cancerous[3].
Is stage 4 colon cancer curable?
Stage IV colon cancer has a 14% relative 5-year survival rate.
Figure: stages of colon cancer
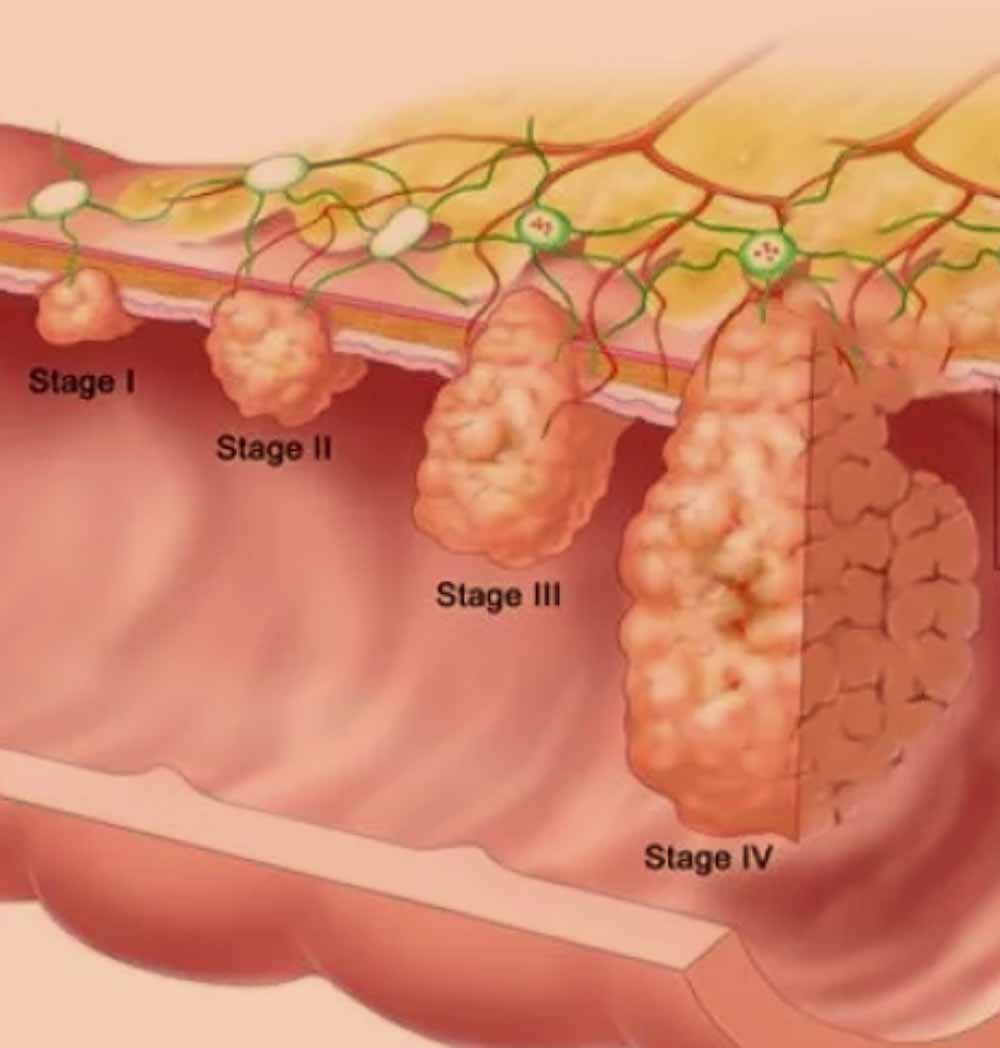
This means that about 14% of people with stage IV colon cancer will survive five years. No one, including your doctor, can accurately tell you how long you will live[4].
Sources and references
Extensive health manual for home use, Youth Book Publishing House
- What Are the Symptoms of Colorectal Cancer? - https://www.cdc.gov
- Colon Cancer Treatment - https://www.cancer.gov
- What Is Colorectal Cancer? - https://www.cancer.org
- What's the Outlook for Stage IV Colon Cancer? - https://www.webmd.com